Health systems around the world face the same fundamental challenge: how to deliver broad access to health services while improving quality of care and controlling costs. Greater competition has often been proposed as a solution that elegantly addresses each element of that challenge.1
There is no consensus, however, as to how much competition is appropriate in health care. Too often, the debate is argued based on strongly held ideological presuppositions or vested interests rather than a dispassionate review of evidence, and thus a full consensus on competition in health care may never be reached. Furthermore, countries differ significantly in the values they hold most important and the goals they have for their health systems. Nevertheless, we believe that by examining the available evidence through the lens of economic theory, it is possible to develop a framework that health systems can employ to decide when and how competition can be used to promote access to high-quality, efficient care.
Our focus here is on competition among providers—most often for patients, but in some cases for payor contracts.2 We suggest that the level of provider competition that is appropriate will vary based on the nature of the clinical services delivered. For highly specialized services, competition should be limited or used only very judiciously to ensure quality and avoid overdelivery. In contrast, greater competition could be an effective mechanism for improving the quality and efficiency of less specialized services, particularly care delivered outside the hospital.
The arguments for and against provider competition
Compelling arguments can be made both for and against provider competition in health care. The strongest argument in favor of competition is that it can be designed and deployed to create potent incentives that encourage providers to innovate so that they can deliver higher quality at lower cost. Porter and Teisberg, for example, have noted that:
In a normal market, competition drives relentless improvements in quality and cost. Rapid innovation leads to rapid diffusion of new technologies and better ways of doing things. Excellent competitors prosper and grow, while weaker rivals are restructured or go out of business. Quality-adjusted prices fall, value improves, and the market expands to meet the needs of more consumers.3
It has also been long known that increased competition among corporations leads to higher productivity.4 Many people, including Porter and Teisberg, have therefore suggested that provider competition could play a similar role in health care, creating the same virtuous circle of innovation, improved quality, and efficiency.
Opponents of provider competition argue that it is inimical to the delivery of good health out-comes at a reasonable cost. Competition, they maintain, often encourages excess capacity and duplication of services, and thus it can lead to supplier-induced increases in demand. Opponents also argue that the markets for some health services are natural monopolies and that care quality will suffer if competition is introduced. Furthermore, they suggest, in at least some health systems, provider competition can promote profit making and market success over patient care; it can also penalize the least well-off patients, thereby exacerbating health inequalities.
At the root of the problem, opponents argue, is the fact that some of the fundamental mechanisms through which competition drives improvements in normal markets do not work in health care. For example, because of the information asymmetry between providers and patients, health care consumers lack an effective way to choose among providers based on care quality. In such a market, competition will not drive up quality. Even proponents of competition recognize that health care suffers from a high number of potential sources of market failure—not only information asymmetry, but also uncertainty, adverse selection, and moral hazard. The combination of these factors makes it difficult for a health care market to function efficiently and, consequently, to reap the full benefits of provider competition.
For countries with public-sector health systems, provider competition raises another concern. Many people in those countries take pride in their public systems and fear that the introduction of provider competition leads inevitably to the introduction of private-sector provision and then to the privatization of health care delivery.
The evidence for and against provider competition
Academic evidence can be cited to support each side of the debate. For example, a recent report demonstrated that increased competition among English hospitals drove up the quality of their management practices, and that, in turn, improved their clinical, operational, and financial outcomes.5 A similar conclusion was reached in another recent paper about English hospitals, which noted that “hospital competition in markets with fixed prices can lead to improvements in clinical quality.”6 In a broad 2006 survey of studies about US hospitals, Martin Gaynor found that for Medicare patients (for whom pricing is fixed), most of the empirical evidence suggests that hospital quality is higher in more competitive markets.7 Daniel Kessler and Mark McClellan also showed that competition among US hospitals can improve care quality and control costs.8
Gaynor admitted, however, that the studies he surveyed did not demonstrate a clear link between competition and hospital quality for patients with private insurance. Because pricing for these patients is not fixed, hospitals can compete on price as well as on quality, and thus it becomes more difficult to detect the impact of competition on quality. Furthermore, a 2002 study found evidence that competition among English hospitals may have worsened the quality of care in the UK National Health Service (NHS) to a small degree.9 A subsequent paper by two of the same authors reported that hospital competition did shorten waiting times, but it also appeared to have reduced care quality (as measured by mortality from acute myocardial infarction).10
McKinsey’s experience working in more than 20 health systems around the world yields examples of situations in which provider competition has resulted in poor outcomes, duplicate costs, and inefficient allocation of resources. We have also encountered health systems that function efficiently without competition. However, we have been most struck by health systems in which provider competition, managed effectively, has improved outcomes and patient choice significantly, while at the same time reducing system costs. Many of these examples are described below. Thus, we began to wonder if the question is not whether provider competition is intrinsically good or bad, but rather whether it is possible to identify specific circumstances in which the judicious use of provider competition is likely to produce the desired results.
How much competition is feasible?
Five core questions need to be considered to establish how much provider competition is appropriate in a given clinical setting (Exhibit 1):

What is the relevant market-segment size?
What is the minimum economic scale?
What is the minimum clinical scale?
Are there significant barriers to market entry or exit?
Are there significant barriers preventing patients from switching providers?
The answer to each question varies considerably depending on the clinical setting, even within a given care pathway.11 As a result, the level of competition that is healthy may also vary considerably in different clinical settings—largely (but not entirely) because of the minimum economic and clinical scales needed to ensure high-quality, efficient care delivery.
Consider, for example, the difference between weight-loss services and bariatric surgery in the obesity care pathway. For providers of weight-loss services (Weight Watchers, Slim-Fast, local gyms, etc.), the minimum economic scale is low: setup and overhead costs are small. The minimum clinical scale is also relatively low: the level of training needed to provide nutritional consultations and programs of physical activity is not as substantial as the level required to perform surgery. Furthermore, no minimum throughput of patients/customers is necessary to ensure that the services provided are safe. As a result, weight-loss services can be delivered by a variety of competitors in most cities and towns.
In comparison, bariatric surgery requires a substantial amount of clinical expertise and specialized infrastructure, as well as a relatively high patient throughput, if high-quality care is to be delivered. A bariatric surgery provider requires a population base of about one million people to ensure that an adequate number of patients will request treatment.
In many cases, minimum clinical scale is the decisive factor for determining how much competition is appropriate. For example, a provider can deliver routine childhood immunization services safely to a relatively small population (perhaps 10,000 or 20,000 people). By contrast, a high-quality inpatient pediatric service that offers 24/7 access to specialist staff requires a much larger population (probably about 500,000 people) to ensure that the staff takes care of enough children to keep its skills sharp. Consequently, a small city could safely support multiple providers of childhood immunization services but only one hospital offering inpatient pediatric care.
We have come to believe that as health care markets become less specialized and less reliant on expensive infrastructure, they can support an increasing number of providers. Pragmatically, this means there should be less competition when care is delivered in highly specialized hospital settings and more competition when care is delivered outside the hospital (Exhibit 2).
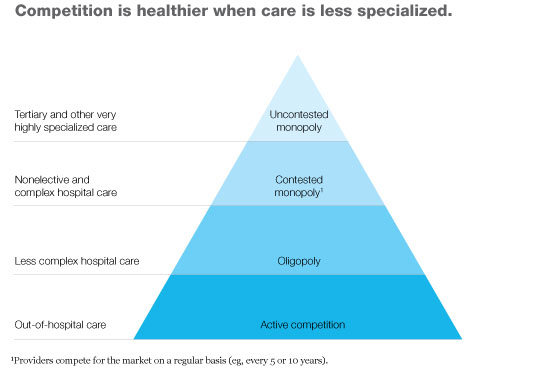
Although this conclusion makes intuitive sense, it has not yet been proved within the health care arena, largely because most of the policy and academic focus in the past ten years has been on competition in the acute sector.12 If the conclusion is true, however, many of the potential gains from increased provider competition are likely to be in primary and community care. Coincidently, this is where most health systems are currently looking for innovation to provide the biggest gains in care quality and productivity.
What is our prescription?
We believe that health systems can use competition judiciously to drive up care quality and control costs by matching the level of competition to the nature of the clinical services delivered. To take advantage of this opportunity, however, most health systems will need to change. Some will first have to alter the structure of their health care markets to make appropriate levels of competition possible. Most systems will need to take steps to enable more effective—and more appropriate—competition, whether within existing or new market structures.
Altering the market structure
Although many health system executives accept the logic of differing levels of competition, some argue that, as a practical matter, changing the competitive structure of a health care market is extremely difficult. We agree. Nevertheless, it is possible, as a number of health systems have shown.
In 2002, for example, Denmark introduced competition by enabling patient choice and amending the health system’s payment structures. If the waiting time for a given treatment exceeded two months in the public-sector health system, patients were allowed to seek treatment free of charge at a private-sector hospital in Denmark or a hospital abroad. The introduction of competition, in effect, increased the system’s capacity; as a result, by 2007 the maximum waiting time in most parts of the public system had been reduced by one-third.13 The improvement in waiting times has enabled the government to tighten its requirements further: patients are now allowed to seek treatment elsewhere if waiting times exceed one month.
The transition to increased competition has not been easy for Denmark, however. To enable patient choice to work, the Danes initially paid private-sector providers a rate above that paid to public-sector hospitals. From an economic perspective, this is understandable—the private-sector providers needed to be compensated for the additional infrastructure required to support the treatments they could now offer patients and for the relative volatility of demand. However, the higher payments created political difficulties for the government. It eventually lowered the reimbursements it paid to private hospitals and created an independent broker, separate from the Ministry of Health, that sets prices for all hospitals.
Queensland, Australia, recently adopted a similar approach to reduce waiting times: its government has contracted with private-sector providers as a way of putting pressure on its public-sector hospitals to improve their performance.14 First-year results suggest that emergency-department waiting times are beginning to shorten in Queensland; however, a decrease in elective-surgery waiting times has not yet been seen.
There are far fewer examples of health systems proactively changing the competitive dynamic in out-of-hospital care, because (as we noted earlier) the primary focus of most efforts has been on the acute sector. Examples do exist, though. In Derby, England, the commissioner brought in a private-sector provider to run a primary care practice.15 Not only did the new provider improve both access to care and the practice’s performance significantly, but it also may have created an important knock-on effect: the threat of private-sector competition appears to have galvanized performance in other nearby practices.
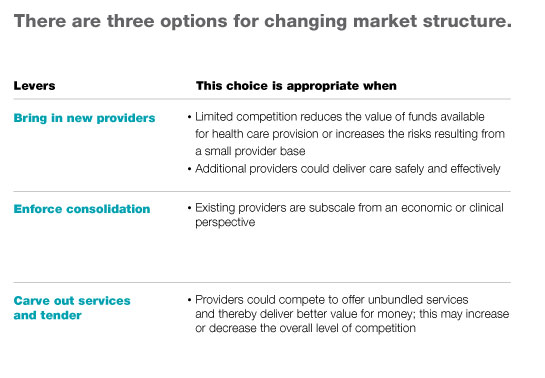
These examples illustrate how health systems have increased provider competition successfully, but it is worth pointing out that in some circumstances, reducing the level of competition may be the wiser course (when care quality suffers because of low patient volumes, for example). Our experience suggests that health systems have three options if they want to change the structure of a health care market: they can bring in new providers to increase competition, enforce consolidation (possibly through mergers or acquisitions) to decrease competition, or carve out specific services and then issue a tender, which can either increase or decrease competition. Which option is best depends on the circumstances a health system faces (Exhibit 3).
Enabling competition
Changing the competitive structure of a market is rarely sufficient on its own to generate the ideal level of provider competition. The system must also take steps to reduce the barriers to competition. Our analyses suggest that six steps can help almost any health system capture the opportunities that provider competition may offer.
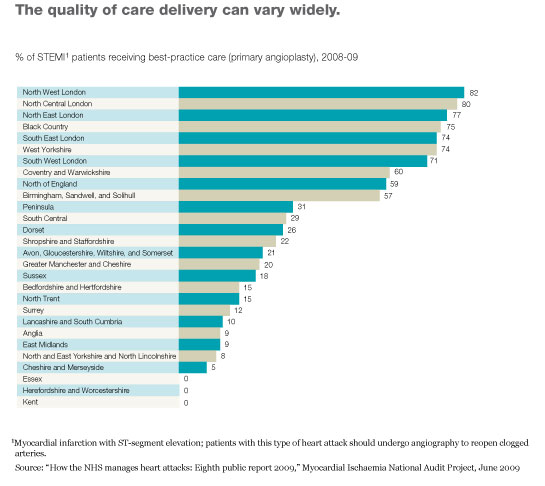
Ensure information availability. Effective functioning of a health system requires accurate data on both the cost and quality of the services delivered. Without this kind of data, it is impossible to spot problems, shift system resources, or identify and disseminate best practices. In many health systems, however, this kind of data is still hard to obtain; it is frequently unavailable for care delivered outside the hospital and sometimes unavailable even for hospital care. Nevertheless, health systems often have more information available to them than they realize, and this information could be used far more effectively to drive performance. For example, the English and Welsh health care systems collect information about the cardiac and stroke services delivered to patients, which reveals stark differences in care quality (Exhibit 4); this information is readily available from credible sources and could be used more aggressively to drive improvements in quality.
Many health systems are beginning to make publicly available the data they do have about health care costs and quality. Because of the data’s complexity, we believe that, in the near term at least, its primary users will be clinicians and payors, not patients (as informed consumers). However, there is clear evidence that even the simple act of measuring data on health outcomes and organizational performance and then making the results publicly available improves the results achieved.16 Improved results can be further guaranteed if data availability is combined with a systematic approach to performance improvement.
Reform reimbursement mechanisms. Reimbursement mechanisms should be designed to ensure that all providers are encouraged to behave in ways that promote the interests of the overall system (for example, they should not be rewarded for offering unnecessary procedures and thereby driving up demand for care). It is also important that funding is linked to and follows each patient; otherwise, providers have little reason to compete with each other for patients. In addition, the reimbursement mechanisms should reward excellence. In an ideal world, providers would receive a quality-adjusted fee based on how their performance influences the outcomes achieved throughout the whole cycle of care, from diagnosis (or even prevention) through to recovery and monitoring. Realistically, this is difficult to do in most health systems today. Nonetheless, health systems have a number of options for ensuring high-quality, cost-effective care throughout a cycle of care. For example, they could use disease-management programs to integrate care for specific conditions,17 institute tariff-based systems that reward quality for bundles of care, and permit payors and providers to share in the value of any productivity gains achieved.
Build primary care capacity and capability. As health systems increasingly attempt to shift the balance of care from hospital to nonhospital settings, much of the competition individual hospitals will face will come not from other hospitals but from non-acute providers. To spark competition both within primary care and between primary care and acute care providers, most health systems will need to increase their primary care capacity to handle higher volumes and to improve the capabilities of their primary care clinicians and managers.
Align incentives for payors. If competitive pressure is to exert the maximum influence on quality and productivity, the purchasers of health services (payors) must have the freedom to buy selectively and be given incentives to seek value for money.
Reduce barriers to patients switching among providers. The ability of patients to change providers can be an important driver of improved quality. In many health systems, patients are discouraged from switching by legal or bureaucratic obstacles, such as geographic restrictions and complex re-registration requirements. Health systems should ensure that patients can change health care providers as easily as they can switch mobile-phone networks.
Reduce barriers to entry and exit. Finally, it is important that health systems reduce unnecessary barriers to market entry and exit. Allowing poor-performing providers to exit the market and high-performing providers to enter it is critical for encouraging innovation and providing incentives for high performance. In some cases, however, market exit may not require a facility’s closure; a change in management may be sufficient to achieve the desired outcome.
What does this mean for care delivery?
As we have shown, the level of provider competition that is healthy varies depending on the clinical setting. Thus, health systems should use different strategies for different types of care.
Highly specialized care
For health services that require a relatively high level of specialization, competition could inadvertently encourage excess capacity and duplication of infrastructure. In developed countries, overcapacity in the acute sector is often more common than undercapacity; introducing new providers would therefore be a mistake.
Health systems should instead seek, whenever possible, to sharpen the competitive dynamic among existing acute care providers. Because many highly specialized services are natural monopolies, multiple acute care providers should not compete to offer those services within a limited geographic area. In some cases, however, the providers could be allowed to compete to become the sole deliverer of a specific service for a fixed period. The winning provider of each service would be issued a license to deliver care for a specified time (perhaps ten years), along with clear outcome-based performance metrics. The remaining providers could focus on other types of acute care, reconfigure themselves to offer lower-acuity services, or simply exit that market. This approach introduces competitive forces into monopolistic markets without risking unnecessary duplication of costs.
Admittedly, for some very specialized services (complex pediatric surgery, for example), even this limited approach to competition may not be feasible. When this is the case, health systems should fall back on regulation and performance management to ensure high-quality care delivery.
Less specialized hospital care
For less specialized acute services, more classic models of competition are usually suitable. Most markets, for example, can sustain a number of efficient and safe providers of elective surgery. Thus, encouraging sharper competition among existing providers or even, in some cases, introducing new providers could yield improved efficiency and better health outcomes.
Before new providers are added, however, it is important that the health system carefully analyze whether the associated increase in system costs will be offset sufficiently by improved productivity and quality. Furthermore, competition for less specialized acute services will not achieve its desired ends unless mechanisms are in place to allow some providers to reconfigure the services they offer or, if necessary, exit the market entirely.
Primary and community care
We believe that the case for encouraging the intensity of competition and the emergence of new providers is clear-cut for care delivered, now or in the future, outside the hospital. This is the area in which competition can be introduced most easily and is likely to have the biggest impact—an important consideration given that, as mentioned earlier, it is the area in which health systems are seeking the greatest improvements in quality and productivity.
Increased data availability could help introduce competition by enabling patients (and, in some cases, referring doctors) to compare the quality of services being offered. Initially, the data could focus on metrics that can be easily gathered and readily understood, such as waiting times and satisfaction scores. Over time, outcome metrics could be added as health systems’ data-collection ability and patients’ level of knowledge rose. In some countries, legislative or regulatory action may be required to make it easier for patients to switch providers, for funding to follow the patients, and for funding to reward excellence. However, a virtuous circle could be established in which competition among providers increases the quality and efficiency of care delivered.
New providers of community-based services can be added in a variety of ways. For example, health systems can increase the number of family doctors they train and/or allow ancillary health providers (nurse practitioners, for example) to offer primary care services. In addition, they can introduce or encourage the expansion of new delivery formats, such as polyclinics, ambulatory surgery centers, retail health clinics, and telephone- or Internet-based care provision. Public-sector health systems can reshape their ownership rules to allow private-sector providers to enter the market.
Finally, some health systems may want to consider stimulating competition for control of certain providers, if they do not already permit such competition. Offering incentives for high-performing providers to take over and turn around low-performing providers can drive up quality and productivity as long as the impact on the overall level of competition in the market is appropriately regulated.
In the past ten years, the focus—among academics and policy makers—has been on introducing competition to the acute sector. However, the potential for competition to drive real improvements in out-of-hospital care has been neglected. We believe that it is time for health systems to shift their focus toward unleashing competition in primary care; that is where competition is likely to make the greatest difference.


